Background introduction ALK gene encodes a transmembrane receptor tyrosine kinase (RTK). The ALK-NPM1 fusion protein was first discovered in anaplastic large cell lymphoma (ALCL). It has been found to mutate, amplify or rearrange in other tumors, including neuroblastoma and non-small cell lung cancer. Chromosome rearrangement is the most common cause of ALK and other genes. Fusion, including ALK/EML4, ALK/RANBP2, ALK/ATIC, ALK/TFG, ALK/NPM1, ALK/SQSTM1, ALK/KIF5B, ALK/CLTC, ALK/TPM4 and ALK/MSN.
Dwarka Sector-7, New Delhi-110075
ALK gene fusion detection probe kit
Probe description
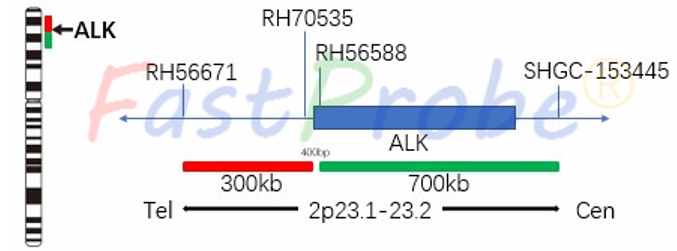
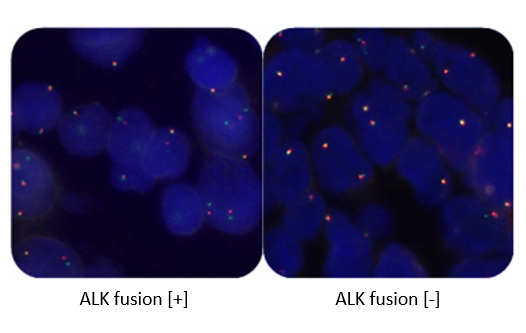
ALK gene break-apart probe uses an orange-red dye to label the 2p23.2 region (3' end), and the green dye to label ALK gene 2p23.1-p23.2 region (5' end). ALK gene break-apart probe detects all ALK gene rearrangements and avoids missed diagnosis by a single fusion gene (such as EML4-ALK). Clinical significance According to the 2013 edition of the Chinese consensus of diagnostic experts on anaplastic lymphoma kinase (ALK) positive non-small cell lung cancer, the positive rate of ALK gene is as high as 30%-42% in NSCLC patients with adenocarcinoma, young (< 60 years old), non-smoking and no mutation in EGFR, KRAS, HER2 or P53 genes. Pathological studies suggest that the positive rate of mucinous or solid adenocarcinomas with signet ring cells is higher than that of other types of lung adenocarcinomas. In 2013, CFDA approved XALKORI (Crizotinib) for targeted therapy of advanced ALK-positive non-small cell lung cancer, and the necessary condition for XALKORI (Crizotinib) drug therapy is FISH for ALK-positive non-small cell lung cancer. Patients with positive ALK gene fusion are sensitive to XALKORI (Crizotinib).

ROS1 (6q22gene) break-apart detection probe kit
Background introduction C-ros sarcoma ROS-receptor tyrosine kinase (ROS1) is located on chromosome 6q22 and encodes a receptor tyrosine kinase (RTK), which is involved in cell growth and proliferation, differentiation and survival. When the ROS1 gene is rearranged, the extracellular region is lost, and the transmembrane region and the intracellular tyrosine kinase region are retained. The rearrangement site mainly occurs in the 32 to 36 exons of the ROS1 gene. In NSCLC, ROS1 gene is mainly fused with SLC34A2, CD74, EZR, SDC4, etc., and continues to activate ROS1 tyrosine kinase domain and downstream signaling pathway, which leads to tumor development.
Probe description
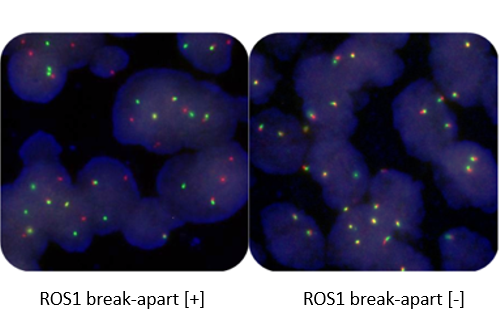
ROS1 gene break-apart probe uses orange-red dye to label the 5' end region of the ROS1 gene, and a green dye to label the 3' end region of the ROS1 gene. ROS1 gene break-apart is able to detect all ROS1 gene rearrangements, avoiding the missed diagnosis caused by a single gene fusion. Clinical significance ROS1 gene rearrangement mainly occurs in young, non-smoking patients with lung adenocarcinoma. ROS1 gene rearrangement is different from other mutations such as EGFR, KRAS, ALK and so on. The positive rate of ROS1 rearrangement was 1.0%-3.4% in NSCLC and 5.7% in EGFR, KRAS and ALK negative population. On March 11, 2016, the FDA approved the indication for XALKORI (Crizotinib) in the treatment of ROS1-positive advanced NSCLC. XALKORI (Crizotinib) indication for ROS1-positive advanced NSCLC have been approved in China. Patients with positive ROS1 rearrangement are sensitive to XALKORI (Crizotinib) drugs.
MET gene amplification detection probe kit
Background introduction MET gene is located on chromosome 7q31.2 and encodes a transmembrane tyrosine kinase receptor. The ligand of MET is hepatocyte growth factor (HGF), which is secreted by mesenchymal cells. The binding of HGF and c-MET can promote cell proliferation, migration, differentiation and morphological changes. The HGF/c-MET signaling pathway is highly regulated and plays an important role in cell proliferation, differentiation and movement.
Probe description
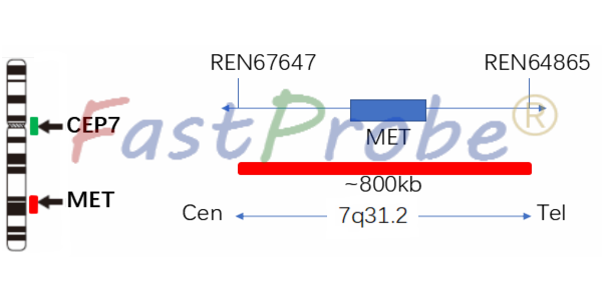
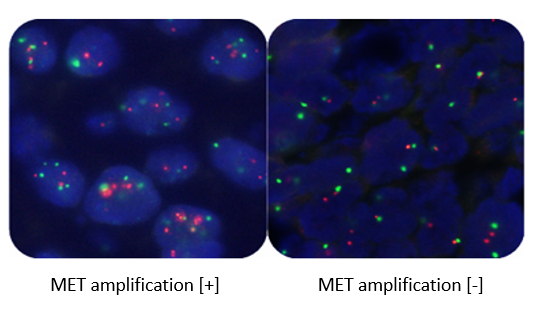
MET gene amplification probe uses orange-red dye to label MET gene region, and green dye to label chromosome 7 centromere region (CEP7). MET gene marker region is located at 7q31.2, and the CEP7 probe is labeled with a specific alpha satellite sequence. Clinical significance MET gene can be amplified in a variety of tumors such as lung cancer, breast cancer, ovarian cancer, thyroid cancer, gastric cancer, colorectal cancer, etc. It is an independent prognostic factor, and the prognosis of patients with MET gene amplification is poor. In NSCLC, MET gene amplification is closely related to poor prognosis and TKIs drug resistance. MET gene amplification is one of the targets of XALKORI (Crizotinib). Tumors in patients with MET gene amplification can shrink significantly after treatment.
RET gene break-apart detection probe kit
Background introduction RET gene is located on the long arm of chromosome 10 and encodes a receptor tyrosine kinase. It is expressed in normal neurons, sympathetic and parasympathetic ganglia, thyroid C cells, adrenal myelocytes, genitourinary tract cells, and testicular germ cells. Activation of the RET protein activates downstream signaling pathways (including RAS, MAPK, ERK, PI3K, AKT, etc.), resulting in cell proliferation, migration, and differentiation. Activating mutations in the RET gene are associated with human malignancies, but if the RET gene loses its function, this can lead to gastrointestinal developmental diseases such as the congenital megacolon or Hirschsprung's disease.
Probe description
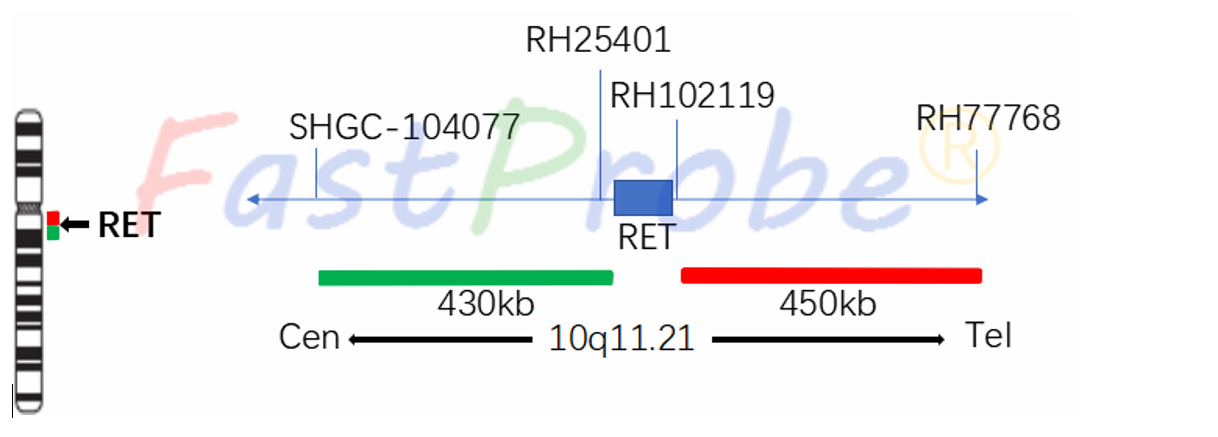
The RET gene break-apart probe uses an orange-red dye to label the RET gene (5'-end) region, and a green dye to label the RET gene (3'-end) region. The RET gene break-apart probe detects all RET gene rearrangements, avoiding missed diagnosis by a single gene fusion. Clinical significance RET gene fusion in patients with non-small cell lung cancer accounts for 1%-2% of the frequency, and the RET gene is mutually exclusive with other driver genes such as EGFR, KRAS, ALK, HER2 and BRAF, i.e., rarely occurs at the same time, the RET gene is an independent gene for driving non-small cell lung cancer. At present, there are four fusion partner genes of RET gene, namely KIF5B, CCDC6, TRIM33 and NCOA4, of which KIF5B is the most important fusion gene, accounting for 90%. RET gene fusion is more common in patients who have never smoked or had adenocarcinoma. Screening of 936 patients with non-small cell lung cancer found 13 patients with positive RET fusion genes, 11 of which were adenocarcinomas (85% probability), and other characteristics of the patients included never smoking, and being younger. Moreover, the primary lesions of these patients are often smaller (100%, less than 3 cm).